XX Genotype
People with genotype XX are chromosomal females (genotype refers to a person’s genetics). However, an XX individual’s gender may differ from their genetics. In this chapter, we will focus on sex, not gender. Therefore, a female is a person with the XX genotype.
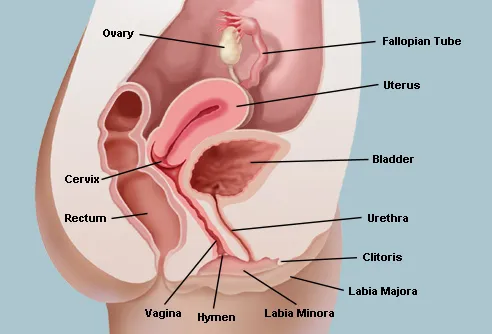
Cisgender Female Anatomy
Ovaries are female gonads. Ovaries make the hormones estrogen and progesterone and are the site of egg production and maturation. The uterus sits above the urinary bladder and is connected to the left and right fallopian tubes(also called oviducts or uterine tubes). On the distal ends of the fallopian tubes sits the ovaries; however, there is a small gap between the ovaries and fallopian tubes. The inferior portion of the uterus sits an opening called the cervix, where sperm move through after ejaculation, and a baby exits the uterus during labor. The vagina, or birth canal, is the tube the penis penetrates during vaginal sex and the canal a baby uses to exit their mother.
The exterior sex characteristics are collectively known as the vulva. There are two folds of skin that surround the vaginal orifice. The labia majora are the thicker outer folds, and the labia minora are the thinner inner folds. Unlike the labia majora, the labia minora are hairless and may extend beyond the labia majora. The clitoris is homologous to the penis and is about a little smaller and size and contains the same erectile tissue. The clitoris function is for pleasure during coitus.
So, what is female circumcision?
It’s a crime against humanity, plain and simple. The WHO (World Health Organization) aptly calls it female genital mutilation, which is analogous to removing the penis. Some consider male circumcision mutilation too, but a male without his foreskin still has most of the highly sensitive nerves that make sex pleasurable. Female genital mutilation removes all the pleasure from sex and can lead to severe physical and mental health conditions. It is a barbaric procedure still practiced today in some areas of the world, leaving more than 200 million living females without a clitoris (that’s five times the population of California, which is greater than ALL of the females living in the U.S.).
The Primary Cisgender Female Reproductive Hormones
A data table enumerates the primary cisgender female reproductive hormones, the organs that secrete them, and their target organs.
| Hormones | Secretory Organ (s) | Reproductive Target Organ(s) | Hormone Type | Hormone’s Effect on Target Organ |
|---|---|---|---|---|
| Gonadotropin-releasing hormone (GnRH) | Hypothalamus | Pituitary gland | Non-steroid | Stimulates the release of FSH and LH |
| Follicule-stimulating hormone (FSH) | Pituitary gland | Ovaries | non-steroid | Oocyte growth (oogenesis) |
| Leutinizing hormone (LH) | Pituitary gland | Ovaries | Non-steroid | Ovulation |
| Prolactin | Pituitary gland | Breasts | Non-steroid | Milk production |
| Oxytocin | Pituitary gland | Uterus, breasts | Non-steroid | Uterine contractions, milk secretion |
| Estrogen | Ovaries | Uterus, breasts, hypothalamus, pituitary gland, | Steroid | The development of breasts, endometrium, and oocytes regulates the menstrual cycle |
| Progesterone | Ovaries | Uterus | Steroid | Prevents uterine contractions, regulates the menstrual cycle |
| Testosterone | Ovaries, adrenal glands, skin, adipose tissue | Vulva, vagina, breasts | Steroid | Libido, maintenance of breast and vaginal health |
Oogenesis
An oocyte is an egg cell, and oogenesis is the production of oocytes. Females make all of the egg cells they will ever have before birth. However, egg cells are immature because they have not completed the process of meiosis (the cell division that makes sperm and eggs). The oocytes remain in a state of suspended animation until puberty. At puberty, oogenesis resumes. Each month about 20 oocytes restart oogenesis, but only one (most of the time) will complete the process and produce a viable oocyte. The mature oocyte ejects from the ovary during ovulation and enters a fallopian tube. If sperm is present in the fallopian tube, the oocyte may become fertilized. A fertilized egg, or zygote, will divide rapidly until it becomes a hollow ball of physically and genetically identical cells called a blastocyst. The blastocyst moves towards the uterus via ciliary movements (it looks like it is crowd-surfed). When the blastocyst reaches the uterus, it implants on the uterine wall, and embryonic development begins. If sperm are not present or the egg is not fertilized, the oocyte will “crowd surf” to the uterus, and the body will discard it when menstruation begins.

| This is the Oocyte Crowd Surfing Down a Fallopian Tube | This is a Fan Crowd Surfing at a Concert |
|---|---|
 |  |
The result of spermatogenesis is four viable sperm. But a sperm cell is the smallest human cell; only its nucleus enters an oocyte during fertilization. An oocyte is the largest cell by volume in the human body. To begin prenatal development requires a lot of space, nutrients, and organelles (a cell’s organs). Due to the oocyte’s size, oogenesis results in only one viable oocyte and three tiny non-viable polar bodies.
Why does oogenesis make polar bodies?
Oogenesis is meiosis, and meiosis’s purpose is to create cells with half the number of chromosomes as the cell that started the division. The only way to halve the chromosome number is to separate the DNA into four cells.
So the polar bodies have the same amount of chromosomes as the oocyte?
Yep. But the oocyte has all the machinery to make a child, which the polar bodies do not.
The Uterine Cycle
A female’s reproductive cycle is 28 days on average (it is very common for teenagers and young adults to have a longer or shorter cycle) and comprises two stages:
- The uterine cycle or menstrual cycle documents the change of the lining of the uterus over the 28-day cycle.
- The ovarian cycle documents the changes within the ovary over the 28-day cycle.
The uterine cycle begins when a woman starts to menstruate (mense). Menstruation occurs when a woman sheds the lining of her uterus through the vagina – commonly called a period or menstrual bleeding. The lining of the uterus is the endometrium. The menstrual phase lasts until the old endometrial layer is removed by day 5. The endometrium begins to rebuild itself when menstruation ceases. The endometrium is the highly vascular lining of the uterus where the embryo and placenta will develop.
After menstruation, the proliferation phase (days 6-14) begins. The ovaries secrete copious amounts of estrogen, which stimulates the rapid regrowth of the endometrium, which is fully developed by day 14.
The secretory phase (days 15-28) begins with reduced estrogen secretion and progesterone spikes. The increase in progesterone prevents uterine contractions. If the uterus contracts prematurely, the endometrium will shed too early (early menstruation).
Why is that a problem?
It takes 6-7 days for the fertilized egg to divide into a blastocyst and reach the endometrium. A female will produce high levels of progesterone for about 10 days if the hormone human chorionic gonadotropin (hCG). If a female sheds her endometrium before or after the blastocyst implantation, the embryo will be discarded with the menstrual flow.
What hCG?
Human chorionic gonadotropin (hCG) is a hormone secreted by the embryo after implantation and tells the ovaries to maintain high progesterone and estrogen levels. Therefore, hCG stops the menstrual cycle so embryonic development can happen.
A few days before menstruation (days 24 to 28), plasma progesterone and estrogen levels drop significantly. The low estrogen environment will cause the “death” of the endometrium, and without progesterone, the uterus begins to contract, which is the cause of menstrual cramps.

Stages of the Uterine Cycle
| Stage | Days | Estrogen and Progesterone Plasma Levels | Primary Events |
|---|---|---|---|
| Menstrual | 1-5 | Low | The uterus sheds the endometrium; menstrual flow |
| Proliferation | 6-14 | Elevated estrogen, low progesterone | Growths of the endometrium |
| Secretory | 15-28 | High then low | Maintenance of the endometrium (first 7-10 days); menstrual cramps and the deterioration of the endometrium in the later stage |
The Ovarian Cycle
The ovarian cycle occurs concurrently with the menstrual cycle. It starts with menstruation and ends when menstruation begins again.
During fetal development, females’ ovaries make about 2 million primary oocytes, and they will never make more. However, at birth, the primary oocytes go into a stage of suspended animation and will remain so until puberty. The primary oocyte is a diploid cell, which means it has 46 chromosomes, the same number as all the nucleated cells in the body. At puberty, about a dozen primary oocytes begin the follicular phase, but usually, one matures enough to become a viable haploid oocyte (containing a half set of chromosomes, or 23 chromosomes).
The follicular phase (days 1-13) is where the primary oocyte completes oogenesis in the ovarian follicle or follicle. The follicles are hormone-rich sacs where primary oocytes develop. The follicle bathes the primary follicle in estrogen, which causes the primary oocyte to complete oogenesis, becoming an ootid (23 chromosomes).

Is the ootid a mature oocyte?
No, the ootid is connected to a polar body. An ootid does not become a mature oocyte until fertilized by sperm. At fertilization, the ootid ejects its polar body and becomes a mature oocyte for a few hours until the union of the sperm and oocyte DNA.
So a mature oocyte only occurs with fertilization?
Yep.
On the last day of the follicular stage, plasma estrogen levels stimulate the hypothalamus to secrete gonadotropin-releasing hormone (GnRH). GnRH stimulates the pituitary gland to secret copious amounts of luteinizing hormone (LH), leading to the LH surge. The LH surge weakens the ovarian wall, and the ootid ejects from the follicle and ovarian wall.
The release of the ootid from the ovary is ovulation. Ovulation occurs on day 14 and is the shortest ovarian cycle phase. The distal end of the fallopian tube contains finger-like extensions called fimbriae. The fimbriae guide the ootid into the fallopian tube via pulse-like motions. If the ootid does not enter the fallopian tube, it will disintegrate in the pelvic cavity. However, in rare circumstances, sperm fertilizes the ootid in the pelvic cavity, and the fertilized oocyte may implant outside the uterus. An ectopic pregnancy is the implantation of a fertilized oocyte on any tissue other than the endometrium. Most ectopic pregnancies occur in the fallopian tubes, but all are fatal to the embryo and are usually life-threatening for the mother.

The luteal stage (days 15-28) is the final stage of the ovarian cycle. The follicle becomes the corpus luteum (yellow body) after ovulation. The corpus luteum secretes estrogen and progesterone, so the endometrium remains vascular and intact for embryo implantation.
So what happens to the corpus lutetium when after implantation?

If implantation of the embryo occurs, the embryo will secrete hCG. HCG stimulates the corpus luteum to remain intact and continues secreting estrogen and progesterone until the placenta develops.
What happens if an oocyte is not fertilized?
The corpus luteum will begin to disintegrate about a week after ovulation. The disintegrating corpus luteum causes plasma estrogen and progesterone levels to drop significantly, and the uterus will prepare for menstruation.
Stages of the Ovarian Cycle
| Stage | Days | Estrogen and Progesterone Plasma Levels | Primary Events |
|---|---|---|---|
| Follicular | 1-5 | Low then high | Primary oocyte develops into an ootid in the follicle; LH surge |
| Ovulation | 6-14 | High | The follicle ruptures, releasing the ootid from the ovary |
| Luteal | 15-28 | High then low | Corpus luteum secretes large quantities of estrogen and progesterone (first week) Corpus luteum disintegrates, and estrogen and progesterone levels drop (last few days) |
Hormone Feedback Loops
The homeostatic feedback loop involved in the ovarian cycle is complex. Below are the feedback loops throughout the ovarian cycle of a female who is not pregnant.
- Early follicular stage (days 1-5)
- Estrogen inhibits GnRH secreting, which results in low LH and FSH secretion
- Plasma estrogen and progesterone plummet, and menstruation begins
- Late follicular stage (days 6-13)
- Low estrogen levels stop the inhibition of GnRH
- GnRH stimulates the release of FSH and LH from the pituitary gland
- FSH increases estrogen secretion, beginning the development of the oocyte in the follicle
- On day 13, rising estrogen levels cause the LH surge
- Ovulation (day 14)
- The LH surge causes a spike in estrogen levels which leads to ovulation
- Early luteal stage (days 15-22)
- The corpus luteum secretes high levels of estrogen and progesterone
- Estrogen completes the development of the endometrium
- Progesterone inhibits uterine contractions
- Late luteal stage (days 23-28)
- Plasma estrogen levels reach their apex and inhibit the release of GnRH
- The corpus luteum disintegrates, causing a dramatic decrease in estrogen and progesterone levels
- The endometrium begins to die, and uterine contractions begin

Menopause
Humans, orcas, and piolet whales are the only placental animals that enter menopause. Menopause is when the ovaries lose their sensitivity to LH and FSH. Without LH and FSH, estrogen and progesterone production levels become so low that the menstrual and ovarian cycles stop.
Why do females experience menopause?
The grandmother hypothesis is the best answer we have, however, it is just a hypothesis. Killer whales, piolet whales, and human mothers usually remain in contact with their daughters until death. Once a female’s daughters have children, they stop menstruating so they can use their energy to support their daughters and grandchildren.
Mammary Glands
During puberty, high plasma estrogen triggers the formation of the breasts. The breast mainly comprises adipose tissue. Deep within the breasts are the mammary glands that secrete milk after the child’s birth. The mammary glands are connected to mammary ducts, which connect to the nipples. During pregnancy, the pituitary gland secretes the hormone prolactin, which starts milk production. Over the nine months of pregnancy, the breasts enlarge as the mammary glands fill with milk. When breastfeeding, the suckling causes the release of oxytocin, which causes milk secretion. The more suckling, the more oxytocin and more secretion. Therefore, breastfeeding is a positive feedback loop.


Urinary Tract Infections
Females are 14 times more likely to get a urinary tract infection (UTI) than males under 60.
Why?
It has to do with the location and length of a female’s urethra. A male’s urethra (20 cm) is involved in urination and reproduction and is five times longer than a female’s urethra (4 cm). Also, the location of the female urethral opening is much closer to the anus than a male’s.
Why do length and location matter?
The shorter the urethra, the less distance bacteria travel to the bladder. Usually, urination will flush out any bacteria in the urethra. However, suppose a woman has not urinated for an extended period. In that case, bacteria can make it to the urinary bladder or ureters (tubes that carry urine from the kidneys to the urinary bladder) and may cause a UTI. Also, the anus contains bacteria generally harmless to the GI tract but can cause infection in the urinary tract.
